Dr. Roberto Leon MD FRCSC (biography and disclosures)
Disclosures: Received an honorarium from Bayer for speaking at CME events on IUDs, and from Allergan for speaking on Lolo and Fibristal. Advisor for Pfizer for Duavive. No direct reference is made to products made by Bayer or Allergan in this article. No conflict of interest. Mitigating potential bias: Recommendations are consistent with published guidelines (Endocrine Society, North American Menopause Society, Society of Obstetrician and Gynecologists of Canada), International Menopause Society)
What I did before
One of the most complex decisions that women (and their physicians) occasionally need to take in mid-life is whether to use prescription medications for their menopausal symptoms. Previously known as Hormone Replacement Therapy (HRT), Menopause Hormone Therapy (MHT) is an effective and evidence based treatment (1) for moderate to severe hot flashes and/or night sweats (defined as bothersome enough to interfere with daily activities, impair quality of life and/or interrupt sleep).
But women fear getting cancer, especially breast, or a heart attack. And certainly, there are risks associated with the consumption of hormones. As a gynecologist, identifying which patients are at a higher risk of complications (and therefore recommending against MHT) has always been a challenge for me. Often it was an educated guess. In most women, however, the benefits outweigh the risks.
There are many great guidelines produced by reputable international organizations such as the Society of Obstetricians and Gynecologists of Canada (SOGC), the North American Menopause Society (NAMS), and the International Menopause Society (IMS), to name a few, but they all contain a large amount of scientific information but with very little practical guidance for everyday use.
What changed my practice
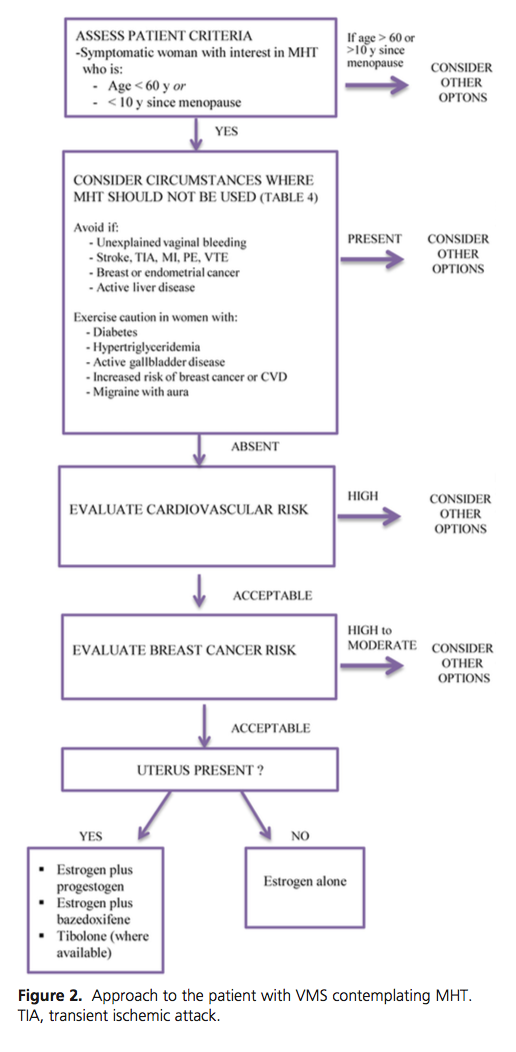
The Endocrine Society published an article in November 2015 (2) with the clearest step by step approach on how to select women for MHT, from a safety point of view (see attach : Flowsheet – Endocrine Society). It has five logical questions which can be answered either directly, or by using an app and a website. MHT can then be recommended to women who are at the right age, have no contraindications, and have low cardiovascular and breast cancer risks.
What I do now
After taking a basic medical history, we reviewed the menopausal symptoms and their possible solutions, including a discussion on lifestyle modifications, over-the-counter medications, cognitive behavioral therapy, acupuncture, and nonhormonal prescription medication. If the patient has tried various nonhormonal methods, and continues to have moderate to severe menopausal symptoms, then I go through the Endocrine Society’s flowsheet to see if it is safe to prescribe MHT.
Question 1: ASSESS PATIENT CRITERIA – IS SHE AT THE WINDOW OF OPPORTUNITY? Age less than 60 years or less than 10 years since her last menstrual period is considered the window of opportunity for initiating MHT. Data from the Women’s Health Initiative (WHI) trial (1,3) showed that if MHT is initiated after 60, it increases the risk of a heart attack and breast cancer. If initiated within the window of opportunity, it is more likely to be protective against cardiovascular disease, and more so if FDA approved bioidentical (FDA approved) transdermal hormones containing estradiol and micronized progesterone are used (4). If the patient is within the window, move to question number 2. If she is more than 60 years old or more than 10 years since menopause, other options should be considered
Question 2: RULE OUT CONTRAINDICATIONS FOR MHT. There are some absolute contraindications such as unexplained vaginal bleeding, stroke, TIA, MI, PE, VTE, breast or endometrial cancer, and active liver disease. Relative contraindications include diabetes, hypertriglyceridemia, active gallbladder disease, increased risk of breast cancer or CVD and migraine with aura (see attached checklist of contraindications to MHT). If contraindications are present, consider other options. If none, moved to question number 3.
Question 3: EVALUATE CARDIOVASCULAR RISK. There are many tools to calculate the CVD risk, such as the American College of Cardiology (ACC)/American Heart Association (AHA) 10-year CVD risk, Framingham and Reynolds. I prefer to use the North American Menopause Society NAMS App (5) called MenoPro, which is based on the ACC/AHA (see attached NAMS questionnaire, assessing CVD risk). It has been validated in women over 45 years with menopausal symptoms. I go through the questions with the patient and enter their response in my tablet or iPhone. It takes about 2-3 minutes. Total cholesterol value and blood pressure measurement are required. Patients can complete it themselves, as there are Health Care Provider or Patient modes, or complete the form (see attached NAMS questionnaire – risk of CVD). The App also contains information on treatment options, and on the various types of hormones, best route of administration, and dose-equivalence of various preparations. Each step of the algorithm should be reassessed at least once a year or if health status changes. If this total score indicates a higher risk than normal, consider other options. For medium risk women, consider transdermal estrogen and move to question number 4. If the risk is low, moved to question number 4.
Question 4: EVALUATE BREAST CANCER RISK. The National Cancer Institute Breast Cancer Risk Assessment Tool provides a standardized online risk calculator for 5-year risk of invasive breast cancer (6) (see attached NCI questionnaire – risk of breast cancer). There is no App currently available for this tool, but the data can be entered online (https://www.cancer.gov/bcrisktool). There are 8 questions which I review with the patient, and enter the answers immediately. Neither a breast exam nor mammography are included in the calculator, but mammography breast density may emerge as an important objective risk for women contemplating MHT. I do request an up to date mammogram, and that they join the mammography screening program of BC if they haven’t done so. If the risk is high, greater than 5%, consider other options. For medium risk women, caution on MHT is advised. If the risk is low moved to question number 5.
Question 5: UTERUS PRESENT? If the answer is yes, estrogen and progesterone should be prescribed. If the answer is no, then estrogen alone is sufficient for the majority.
All the International organizations mentioned above support the use of MHT for the shortest period, (usually 3-5 years) and the lowest possible dose (of estrogen). After five years, the patient should be counselled about tapering down the dose or stopping it all together, mostly because of the lack of studies establishing long-term safety. In a patient chooses to continue, understanding this lack of information, I am happy to prescribe it for longer than five years.
The US Task Force for Disease Prevention is collecting data about the long-term administration of MHT, not only for menopausal symptoms but to also to decrease the incidence of chronic diseases such as osteoporosis, cardiovascular disease and dementia that may be linked to the low estrogenic environment after menopause. At present, there is no scientific support for this approach, but the US Task Force is planning to release an updated guideline in 2017 (7). Stay tuned.
I would like to add, as it is very important for safety:
Question 6: IS THE PATIENT ON ADEQUATE DOSES OF PROGESTERONE? I have recently seen a few cases of endometrial cancer in women who are on estrogen but are receiving insufficient doses of progesterone. A survey by Gass et al (8) revealed 4 cases of endometrial cancer out of 326 women using compounding hormone therapy in the USA.
Regardless of the dose of estrogen, or the route, certain basic conditions apply for the added progesterone:
- The transdermal absorption of progesterone is erratic, and the progesterone cream is not sufficient for endometrial protection.
- Medroxiprogesterone acetate (Provera) and other synthetic progestogens have a good protective effect, but they are likely to have a negative impact on breast cancer risk and metabolic parameters (and hence CVD events) (2).
- Most organizations recommend micronized progesterone (Prometrium) at 100 mg PO HS daily (9). Sequential use of 200 mg 14 days a month can also be employed, but it is less popular because many women will have a menstrual cycle at the end of the 2 weeks.
Women who cannot tolerate 100 mg, but do well on 50 or 75 mg of micronized progesterone, should be offered a yearly transvaginal ultrasound to measure the thickness of the endometrium (please note that a transabdominal ultrasound is not as accurate) and/or yearly endometrial biopsies. Progesterone does not eliminate the risk of endometrial cancer completely (10). If there is any bleeding, a full gynecological assessment is mandatory.
Resources:
- Flowsheet Endocrine Society: view
- Check list: contraindications for HRT: view
- NAMS questionnaire – risk of CVD): view
- NCI questionnaire – risk of breast cancer: view
References:
- Langer DA. The evidence base for HRT: what can we believe? Climacteric. 2017;20:2,91-96. (Request with CPSBC or view UBC) DOI: 10.1080/13697137.2017.1280251
- Stuenkel CA, Davis SR, Gompel A, et al. Treatment of symptoms of the menopause: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2015;100:3975-4011. (View with CPSBC or UBC) DOI: 10.1210/jc.2015-2236
- Hodis HN, Collins P, Mack WJ, Schierbeck LL. The window of opportunity for coronary heart disease prevention with hormone therapy: past, present and future in perspective. Climacteric. 2012;15:217-228. (View)
- Simon JA. What’s new in hormone replacement therapy: focus on transdermal estradiol and micronized progesterone. Climacteric. 2012;15:3-10. (Request with CPSBC or view UBC) DOI: 10.3109/13697137.2012.669332
- Manson JE, Ames JM, Shapiro M, et al. Algorithm and mobile app for menopausal symptom management and hormonal/non-hormonal therapy decision making: a clinical decision-support tool from The North American Menopause Society. Menopause. 2015;22:247-253. (View with CPSBC or UBC) DOI: 10.1097/GME.0000000000000373
- National Cancer institute. Breast Cancer Risk Assessment tool. https://www.cancer.gov/bcrisktool. Updated on May 18, 2011. Accessed on February 26, 2017. (View)
- US Preventive Services Task Force. Final Recommendation Statement: Menopausal Hormone Therapy: Preventive Medications. 2012. https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/menopausal-hormone-therapy-preventive-medication. Updated December 2016. Accessed on February 26, 2017. (View)
- Gass MLS, Stuenkel CA, Utian WH, et al. Use of compounded hormone therapy in the United States: report of The North American Menopause Society Survey. Menopause. 2015;22:1276-1285. (View with CPSBC or UBC) DOI: 10.1097/GME.0000000000000553
- Gompel A. Micronized progesterone and its impact on the endometrium and breast vs. progestogens. Climacteric. 2012;15:18-25. (Request with CPSBC or view UBC) DOI: 10.3109/13697137.2012.669584
- Baber R, Panay N, Fenton A, IMS Writing Grp, IMS Writing Group. 2016 IMS recommendations on women’s midlife health and menopause hormone therapy. Climacteric. 2016;19:109-150. (Request with CPSBC or view UBC) DOI: 10.3109/13697137.2015.112916

{kind=link}
Thanks for this information, Dr. Leon. It sounds like a practical & useful approach to MHT. Further on this topic, recently one of my patients brought the CeMCOR (The Centre for Menstrual Cycle and Ovulation Research, http://www.cemcor.ubc.ca) website to my attention, as she wanted to be on progesterone as well as estrogen despite having had a hysterectomy – this was a new concept for me. For those who don’t know, CemCOR was founded by Dr. Jerilynn Prior, whose name many of us recognize (she was one of my lecturers in medical school in the late 1980’s). The website has areas for patients and healthcare providers. It’s worth a look.
Thank you for the information Dr Leon. I am definitely going use this approach in my practice.
I think the 5 question approach Is a useful guide in deterimining eligibility for MHT.
Thank you I did appreciate this article as well and encouraged to return to more HRT use with a strong approach. I wonder about the use of progesterone only in perimenopausal woman. It seems to work well for symptoms. Would progesterone only hold any benefit for menopausal women?
Thanks, very helpful and straightforward article. I wonder about small doses of vaginal estrogen (i.e. estrace cream).
I had been told no need to also rx progesterone, but should we still have the woman on both estrogen and progesterone in this case?
useful article
Diana (and Christine): thanks for the info Diana. I know Dr Prior has always been keen on using progesterone. I see no harm from using micronized progesterone. Medroxiprogesterone acetate appears to increase proliferation of breast cells (and hence breast cancer), and affect the lipoproteins in a negative way, so I wouldn’t use it if the patient had a hysterectomy. Thanks for the referral to her website. She seems to make a good point, i.e., progesterone increasing MBD for using it.
Jenna: the table didn’t come out formatted. I hope it clarifies your question. The intermediate dose is optional. I discuss it with the patient. If they are at high risk for endometrial cancer, I strongly recommend it. Problem tends to be the cost more than anything else, as women feel good (not all) on the progesterone. They sleep better too.
If local estrogen is prescribed, the need for progesterone is dose-dependent:
Dose Estrogen Frequency Added Progesterone
Low Vagifem 10 Twice a week Not required
EstRing Q 3 months
Intermediate Premarin 0.5 gm Twice a week Controversial
Estragyn 0.5 gm Twice a week
High Premarin >0.5 gm Twice a week Highly recommended
Estragyn >0.5 gm Twice a week
Thank you for this great summary. I wonder if you can you comment on the use of Mirena (or similar) IUD/IUS. Specifically, is the progesterone level in the device sufficient or appropriate to balance an estrogen given in MHT? The Levonorgestrel level in Mirena is variable, obviously declining over the 60 month period of use. The product monograph states that it creates a stable plasma level of 150-200pg/ml. The levels measured in the endometrial tissue reported in the monograph are from a very small sample size (N=6!) but they report the levels being 808ng/ml.
Hi Jillian:
Good question but I retired 4 years ago and I’m not in a position to comment. But thanks for your kind words and good question.
Roberto Leon